

 The diagnosis of Multiple Sclerosis (MS) requires a very careful and individualized approach, especially because MS can present with a variety of symptoms and because it can mimic a variety of different conditions. Now that immunomodulating therapies are available to help prevent the progression of symptoms and long-term disability, it is more important than ever to try to make the diagnosis as early as possible. Also, because the diagnosis is likely to include the recommendation to take an immunomodulating drug for many years with all of its potential side effects, it is important that the diagnosis be accurate.
The diagnosis of Multiple Sclerosis (MS) requires a very careful and individualized approach, especially because MS can present with a variety of symptoms and because it can mimic a variety of different conditions. Now that immunomodulating therapies are available to help prevent the progression of symptoms and long-term disability, it is more important than ever to try to make the diagnosis as early as possible. Also, because the diagnosis is likely to include the recommendation to take an immunomodulating drug for many years with all of its potential side effects, it is important that the diagnosis be accurate.
The most important method in making the diagnosis of MS is a careful history and examination. For the relapsing remitting form of MS, the individual attacks should build for a period of time, be stable, and then spontaneously improve. Sometimes they return to normal but sometimes they do not fully recover.
When the diagnosis is made in this clinical manner, tests are used to rule out diseases that mimic MS and to obtain baseline information to later judge the effectiveness of therapy. In order to diagnose patients and start them on therapy sooner, the neurologist is under a lot of pressure to make the diagnosis with the first clinical attack rather than waiting for multiple attacks to occur. In 2001, new criteria was adopted for the diagnosis of multiple sclerosis. This criteria is somewhat technical in nature but its use helps to ensure a proper diagnosis. This is accomplished by including criteria to prevent over-interpretation of laboratory information and a reminder to the neurologist to consider, on a case-by-case basis, diseases that at times resemble MS. These diseases include Lyme disease, vasculitis (an inflammation of blood vessels), sarcoidosis, syphilis, and vitamin B12 deficiency, among others.
Classically, MS has been defined clinically as two or more attacks separated in time and space. An attack is a group of neurological symptoms that come on together, usually over a relatively short amount of time but patients typically do not present with multiple symptoms immediately (unless the patient wakes up in this manner). The neurological symptoms have to be objectively verified by the neurologist (either by exam or a visual evoked response). Having two or more attacks in different parts of the brain (separated in space) at different times (separated in time) define MS. If a patient gives a history of two or more attacks and the neurologist can only find objective evidence of one attack, then a diagnosis of MS can still be made with a single MRI that demonstrates dissemination in space, or an MRI with at least two lesions felt compatible with MS and a cerebral spinal fluid (CSF) analysis showing either oligoclonal bands or an increased IgG index.
Dissemination in space on a single MRI requires lesions in different parts of the brain. The CSF change of oligoclonal bands or elevated IgG index indicates an immune response in the central nervous system.If a patient has a single attack but clinical exam suggests two or more lesions, then the diagnosis of MS can be made by an MRI that shows dissemination in time. Dissemination in time means a lesion on MRI more than 3 months after the attack (if enhancing, i.e. the lesion is brighter after administration of an IV agent called contrast) or two MRIs with different lesions more than 3 months apart if there is no enhancing lesion on the first scan.
The most difficult patients to assess are those with a single attack and objective evidence of only a single lesion on examination. This is known as a "clinically isolated syndrome" (CIS). Under the new criteria, these patients can be felt to have MS if their MRI shows dissemination in space or if they have a MRI with two or more lesions consistent with MS and positive CSF findings. Again, the criteria attempts to balance the need to start patients on treatment who ultimately would be diagnosed as MS with the need to prevent treatment of patients who would never develop clinical MS.
Another group of patients have a form of MS that is known as primary progressive MS. These patients do not suffer distinct attacks but rather slowly decline in their neurologic function over time. The criteria for these patients require positive CSF, dissemination in space by MRI, and dissemination in time on MRI or continued progression for one year.This is the most difficult form of MS to be diagnosed early and many of these patients will have difficulty for years to determine their diagnosis.
![]()
The most important way to follow a patient with multiple sclerosis and to make the diagnosis of multiple sclerosis is with a careful history and examination. Laboratory tests can be useful in the setting of confirming the disease, measuring disease burden, and explaining unusual findings in a particular patient.
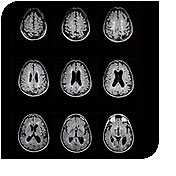
The most useful test at this time to confirm the diagnosis of multiple sclerosis and to get a sense of the burden of disease is the MRI of the brain or magnetic resonance imaging. MRI works for brain tissues because of the high percentage of water in the various brain compartments and the varying degree of movement that they have. Since water is an electrical dipole, when placed in a magnetic field, they line up along the magnetic field. Radio waves are then used to push these molecules sideways and their return to their prior position is detected. Settings on the machine can be varied which allows one to look at the brain on various planes and to bring out different characteristics. Each series of pictures of the brain is called a sequence and a combination of sequences are performed at each MRI setting. Most commonly a contrasting agent called gadolinium or Gad is used to highlight areas where the blood brain barrier is actively disrupted.
In drug studies, MRI are frequently performed to supply additional information. This provides increased power to the study but this is not particularly useful in an individual patient. Over time, brain atrophy is a very useful measure but one which is not readily accessible at this time in a general clinical setting.
While MRI is the most useful ancillary test in a patient with Multiple Sclerosis, it is also responsible for most of the patients who are misdiagnosed with MS as well.
A lumbar puncture, or spinal tap, is the procedure used to obtain fluid that is around the spinal cord. This fluid is made in the ventricles of the brain and circulates through the brain and then some of it goes around the spinal cord. The tests performed on the spinal fluid look for evidence of an inflammatory response in the central nervous system of the type typically seen in MS. These tests are called the IgG index, IgG synthesis rate, and the presence or absence of oligoclonal bands. Other CNS infections and inflammatory diseases can make these tests abnormal but it is a very useful test in the clinical setting if trying to decide if one has MS or not. It is not a useful test at this time to follow patients along. The lumbar puncture can be performed either in a typical patient examination room or with fluoroscopic guidance in a radiology suite. Patients of Dr. Loftus who have had both procedures generally prefer the one performed in a regular exam room. The only frequent side effects of a lumbar puncture or spinal tap is local back pain for a day or two and a post-spinal headache.
There are two different type of needles that can be used. Atraumatic needles cause fewer post spinal tap headaches and are therefore preferred to the more frequently used quickie® needles. The atraumatic needles are relatively newer and have not yet made it into widespread use.
Evoked potentials, and particularly visual evoked potentials are useful tests in the diagnosis of MS. For reasons that are not clear, the small portion of the optic nerve between the eye and where the 2 optic nerves join at what is called the chiasm is frequently affected in MS. Because even a healed MS lesion in this area causes slowing of nerve conduction, the visual evoked potential or visual evoked response is a very useful test. In this test, the patient looks at a checkerboard pattern which alternates the black and white squares. The time is takes for the pattern to change to the change of the EEG over the occipital lobe of the brain (where the pattern is transmitted) is measured. If one eye is substantially slower than the other eye, then there must be a problem with the eye, the retina, or the optic nerve itself. An eye exam can rule out difficulty in the eye and retina leaving the problem in the optic nerve. In the proper clinical setting, it therefore becomes a very useful test. Similar evoked potentials or evoked responses can be performed with hearing and on the nerves on the arms and legs but are not nearly as useful.
Hopefully in the future a blood test for MS can be developed from the current research going on with Tcell vaccination.